(From Alyssa): Through our two years in Kenya, we certainly were reminded daily of the gaps in our medical knowledge regarding tropical medicine and diseases, surgeries, etc. outside the scope of our American residency programs. We learned a lot from our Kenyan colleagues, from the long term missionaries, and from various continuing medical education activities. And thankfully God continued to show His strength in our weaknesses!
From a human perspective, so much additional training would be helpful for our work in Burundi - medical education, various subspecialties, community health, hospital administration, laboratory set up, ultrasound, seminary, etc., etc. For now we're all pursuing linguistic and cross cultural adaptation training (as mentioned in previous and future blogs at Mission Training International in Colorado), Sonship (Gospel transformation discipleship course), language learning (French and Kirundi), and Eric and I are participating in tropical medicine courses at two different sites this year. We look forward to seeing the partners God brings across our paths who have expertise in areas we lack and also to continuing to learn reliance on Him through our deficiencies.
All that to say, I'm currently in Peru for two months at the Gorgas Tropical Medicine course (see my blog on the right for more info & pictures about that) and I bring back to the McCropder blog the Case of the Week:
 |
| Half of my Gorgas classmates pictured with nurses from the clinic we visited this week |
I don't know all the details, but the patient is a 19 year old male who's already been treated for tuberculosis once before. Maybe he had drug resistant tuberculosis in the beginning, maybe he failed to take his medicines as instructed, maybe he couldn't afford transportation to the clinic (TB medicines are free in Peru and in many other countries including Kenya and Burundi - provided by the global fund, the governments, etc., but transportation is still an issue for many people), maybe he has HIV and TB and it was too complicated to visit both clinics (at two separate locations), maybe he recovered but then was reinfected with TB from another source living in his community. I do know he lives somewhere on this hill (below picture taken from the vantage point of the clinic)- very crowded living conditions, very impoverished, ideal for spreading TB to the many close contacts around him.

So he has active pulmonary tuberculosis again. And this time, drug
susceptibility testing was done. And as you see in the below medical chart,
his tuberculosis is resistant to all but one of the first line TB
drugs.
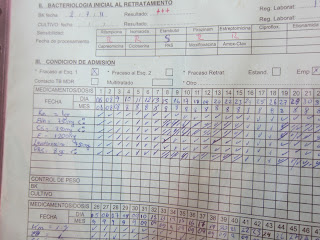 |
| Note the top of the picture: Smear positive tuberculosis resistant to almost all of the most used TB drugs - rifampin, isoniazid, pyrizinamide, and streptomycin |
In the developed world, drug susceptibility testing (which is quite expensive and labor intensive) is done on every patient diagnosed with TB. That way the clinician knows exactly what drugs will work for the individual patient. Developing countries don't have that luxury, so they start with the first line drugs and then if the patient fails treatment or gets TB again, they try to do the specialized testing (of course the resistant patient is likely contagious throughout these months of inadequate treatment). I looked up the statistics for Kenya - 69% of their
retreatment patients get drug susceptibility testing, although the goal is 100%. So many variables are at stake, there - one simple thing, the special bottle to collect the specimen to send to Nairobi for the testing frequently seemed to be out of stock when we were there.
This box contains the entire treatment course for our 19 year old patient. He comes daily for his medications including one injectable med and five oral meds. If he doesn't show up, someone from the clinic goes looking for him - and hopefully finds him unless he gave the wrong address (which is evidently common). This box of meds for one case of multidrug resistant TB costs about $5000. An entire 6 month course of first line meds for a susceptible TB patient costs about $20.
 |
| Our patient's daily six drug regimen |
 |
| Map of the world with proportion of tuberculosis cases per country |
As you can see from the above map, the countries with the most TB include the poorest countries in the world. Of the 22 countries containing 80% of all the tuberculosis cases in the world, Kenya is ranked 13th. I couldn't find the data for Burundi except to find a study from 2003 that reported, "Levels of drug resistance in Bujumbura [Burundi capital city] are higher than average for
Africa, despite long-term use of the DOTS [Directly Observed Therapy] strategy with FDCs [Fixed Drug Combinations] and a ban
on sales of TB drugs."
It's estimated that worldwide only 7% of all multi-drug resistant TB cases are diagnosed (due to a lack of laboratory facilities, rapid tests, funding, etc.). But if you're a ministry of health official for a poor country and you can treat 250 susceptible tuberculosis patients for the price of 1 drug resistant patient, where do you put your efforts?






No comments:
Post a Comment